
A client has Marfan syndrome—what does it mean for him? And what does it mean for massage? Listen in as we review what autosomal dominant means, and we enjoy some new vocabulary: dolichostenomelia (abnormally long, thin limbs) and arachnodactyly (spider-digits). We also learn about the potentially life-threatening complications of this genetic disorder.
Resources:
Inna, Prashanth. “Marfan Syndrome (MFS)." June 18, 2020. https://emedicine.medscape.com/article/1258926-overview.
John Hopkins Medicine. “Marfan Syndrome.” Accessed April 7, 2021. www.hopkinsallchildrens.org/Patients-Families/Health-Library/HealthDocNew/Marfan-Syndrome-(1).
Loeys, B. L. et al. “Differential Diagnosis of Marfan Syndrome.” Adapted from “The Revised Ghent Nosology for the Marfan Syndrome.” Journal of Medical Genetics 47 (2010): 476. Accessed April 7, 2021. www.uptodate.com/contents/image/print?imageKey=CARD%2F59476&topicKey=CARD%2F8150&source=see_link.
The Marfan Foundation. “What is Marfan Syndrome?” Accessed April 6, 2021. www.marfan.org/about/marfan.
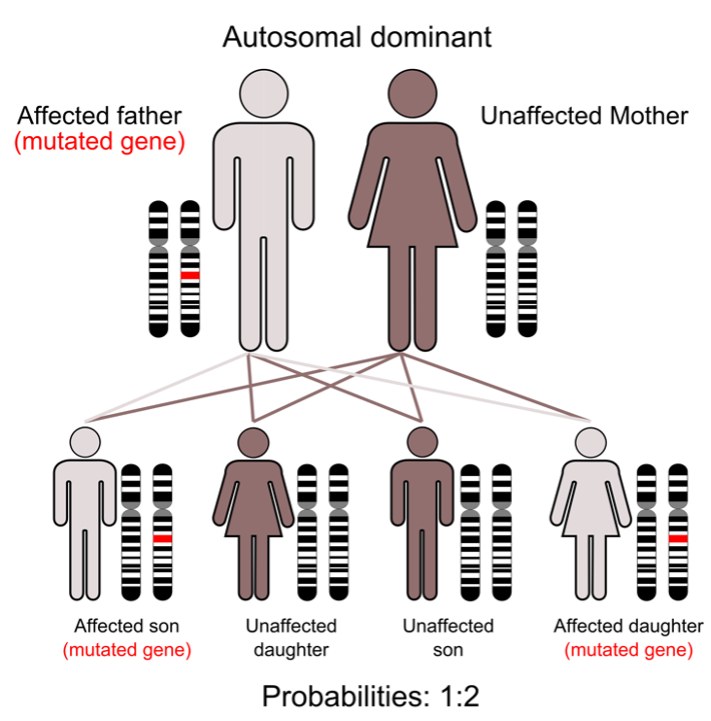
https://commons.wikimedia.org/wiki/File:Autodominant_en_01.png


This podcast sponsored by:
About Anatomy Trains:
Anatomy Trains is a global leader in online anatomy education and also provides in-classroom certification programs forstructuralintegration in the US, Canada, Australia, Europe, Japan, and China, as well as fresh-tissue cadaverdissectionlabs and weekend courses. The work of Anatomy Trains originated with founder Tom Myers, who mapped the human body into 13 myofascial meridians in his original book, currently in itsfourthedition and translated into 12 languages. The principles of Anatomy Trains are used by osteopaths,physicaltherapists,bodyworkers,massagetherapists,personaltrainers,yoga,Pilates,Gyrotonics,and other body-minded manual therapists and movement professionals. Anatomy Trains inspires these practitioners to work with holistic anatomy in treating system-wide patterns to provide improved client outcomes in terms of structure and function.
Website:anatomytrains.com
Email:info@anatomytrains.com
Facebook:facebook.com/AnatomyTrains
Instagram: instagram.com/anatomytrainsofficial
0:00:00.0 Speaker 1: Ruth Werner's best-selling book, a Massage Therapist's Guide To Pathology, is a highly regarded comprehensive resource that sets the standard for pathology education. Written for massage therapy students and practitioners, this groundbreaking resource serves up a comprehensive review of the pathophysiology, signs, symptoms and treatment of more than 500 diseases and disorders. Learn more at booksofdiscovery.com.
0:00:32.7 Speaker 2: Anatomy Trains is excited to invite you to another exciting two-day dissection livestream specialty class, Deep Dive Into Joints, April 24th and 25th. This advanced dissection livestream education experience is presented by Tom Myers and master dissector, Todd Garcia. In this two-day event, we will examine the blended nature of support for each of the joint areas. This special dissection livestream format allows us to explore more deeply, subjects and areas of interest. Visit anatomytrains.com for details.
[music]
0:01:13.6 Ruth Werner: Hi, and welcome to I Have A Client Who, pathology conversations with Ruth Werner. The podcast where I will discuss your real life stories about clients with conditions that are perplexing or confusing. I'm Ruth Warner, author of A Massage Therapist's Guide to Pathology. And I have spent decades studying, writing about, and teaching about where massage therapy intersects with diseases and conditions that might limit our client's health. We almost always have something good to offer, even with our most challenged clients, but we need to figure out a way to do that safely, effectively and within our scope of practice. And sometimes, as we have all learned, that is harder than it looks.
0:02:00.8 RW: Today's story comes from a massage therapist in Michigan who shares this. I had a client come in with a gift certificate. I only saw him once. He was a 40-year-old male who was born with Marfan syndrome, which became more noticeable as he grew. His arms and fingers are longer than normal for his frame. His bones break easily. His right ankle broke two years ago and he's been hit by cars twice. He has mild scoliosis and does push ups in different ways for exercise and physical therapy. He also has a latex allergy. I've only seen him once, so that's all I know so far. He wanted to relax and de-stress with light to moderate pressure. He wanted a special attention to his lats and shoulders and low back.
0:02:45.0 RW: Cool. So here's a client who I learned when I followed up with this massage therapist, didn't really have any special pain or challenge related to his condition. But it does affect the way he functions and his bone density. And that picture about not having big symptoms related to Marfan syndrome, that may change depending on how severely he's affected. But it sounds like he's taking steps now to stay healthy. So let's talk about Marfan syndrome because well, this client didn't seem to have a big effect on his health. For many people, it does, in some surprising and some really serious ways. But before we do that, let me just invite you to send me your I Have a Client Who stories. You can do that in a couple of ways. You can send them to me in an email at ihaveaclientwho@abmp.com, that's ihaveaclientwho, all one word, all lowercase @abmp.com. Alternatively, you can reach out to me through my website at ruthwerner.com or my professional Facebook page, which is called Ruth Werner's Pathology Page, and I will look forward to hearing from you.
0:04:01.5 RW: Marfan syndrome is named for Antoine Marfan, a French doctor who first described it in 1896. It's an inherited autosomal dominant genetic condition. And that means if both parents have this gene, all of their children will have Marfan syndrome. And if only one parent has this gene, each child has a 50% risk of having Marfan syndrome. Does that sound confusing? I'll include a graphic from Wikimedia in the show notes that may help to clarify autosomal dominant genetic conditions. I always have to revisit this stuff about autosomal dominant and autosomal recessive genetic disorders. The genetic anomaly that we see with Marfan syndrome is a problem in the creation of a connective tissue protein called fibrillin. This is a protein that's produced by fibroblasts and it exists in the extracellular matrix, think fascia and supportive connective tissues, and it coordinates the deposition of elastin fibers.
0:05:07.0 RW: Marfan syndrome can range from mild to severe, depending on the extent of the genetic anomaly. It might be identified during childhood, or when teens start becoming really athletic, or in adulthood. It affects men and women equally. And in the United States, we see it in about one out of every 5000 people. Okay, so here's a genetic anomaly in which elastin doesn't lay down properly. So what's the big deal? Well, there are three main ways that this can cause big problems. Marfan syndrome can affect the skeleton, the eyes and the cardiovascular system, along with a few other tissues, but we'll look just briefly at each of these big three. First, let's look at how Marfan syndrome affects the skeleton.
0:05:57.5 RW: Fibrillin and elastin are both required for healthy bone formation. When fibrillin doesn't work well, a number of things can happen. For instance, one of the most common presentations for Marfan syndrome is a person who's really tall with extremely long limbs and long fingers and toes. The technical terms for these are pretty fun. The condition of having unusually long arms and legs is dolichostenomelia. Word geeks like me will be happy to learn that this comes from the Greek dolichos, for long, steno, for narrow, and melia, which refers to a condition of the limbs. And having long fingers is called arachnodactyly, literally spider digits. One casual test for Marfan syndrome is the wrist test. People with this condition can often overlap their thumb and their little finger when they encircle their wrist.
0:07:00.9 RW: But the effect of Marfan syndrome on the skeleton doesn't stop there. People with this disease often have an unusual growth pattern affecting their sternum, it can protrude, which is called pectus carinatum, or it can do the opposite it can sink into the chest and this is called pectus cavus or pectus excavatum. Both of these can be uncomfortable and surgically corrected, but pectus excavatum in particular can really limit the mobility of the thorax and this leads to breathing problems, lung problems and pneumonia. The face of people with Marfan syndrome is often very long and thin and their eyes are set deep and their teeth may be really crowded because their maxilla and mandible tend to be quite narrow. And as we see in the client that is described today, it can cause scoliosis and easily broken bones. Ligament laxity can also contribute to musculoskeletal injury. In fact, Marfan syndrome and the signs and symptoms of Ehlers-Danlos Syndrome often overlap and it can be difficult to distinguish one from another.
0:08:08.8 RW: One final issue is that weakness in the bony connections of the hind foot, that's the heel and the posterior part of the metatarsals, can cause a situation called hind foot valgus. The heel veers outward and the rest of the foot compensates in constant eversion, while the arches appear to collapse. Marfan syndrome can affect the eyes by weakening the elastin that supports eye structures. And this means patients may have myopia, which is really bad nearsightedness, astigmatism, strabismus, glaucoma, cataracts, detached retinas, and dislocation of the lens.
0:08:51.0 RW: And lastly, and most importantly, Marfan syndrome can have a serious, even life threatening effect on the cardiovascular system. These changes in connective tissue because of faulty fibrillin means that the strength and integrity of the heart valves and major blood vessels may be compromised. For instance, Marfan syndrome can cause the mitral valve to not close well. It might prolapse, and that means that the heart has to work much harder or it works less efficiently, and we have arrhythmia and shortness of breath. Damaged mitral valves can also leak so that blood will regurgitate back into the left atrium from the ventricle. The aortic valve, which is the doorway that separates the heart from the aorta, can also become weak and this is even more serious. A weak aortic valve is also associated with problems with the aorta, and enlarged aorta is a common complication of Marfan syndrome, and it can lead to aortic aneurysm.
0:09:53.3 RW: So you might remember that an aneurysm is a bulge in a blood vessel, usually an artery 'cause the pressure is much higher here. Aneurysms can also form in the walls of the heart. People with Marfan syndrome are particularly at risk for this problem because their blood vessels are generally not capable of withstanding the same kind of force as people who do not have this genetic mutation. People with Marfan syndrome may also experience a situation called aortic dissection, and this is where the walls of the aorta may split. And if it's not dealt with, the aorta may actually rupture, which of course, means massive internal bleeding, and death. Fortunately, aortic dissections are really painful, so they don't happen silently, people know. If a person develops an aortic dissection in the ascending aorta, which is the most common way that this happens for people with Marfan syndrome, this requires immediate surgery. If a dissection happens in the descending aorta, this could be managed with medication and monitoring.
0:10:57.3 RW: Until fairly recently, the life expectancy for someone with Marfan syndrome was pretty short, around age 40, because most patients died from something to do with their cardiovascular system. Nowadays, when Marfan syndrome weakens the blood vessels, patients are prescribed beta blockers, and these medications reduce the force of the heartbeat. And this means the heart doesn't have to work so hard, and neither does the aorta. So life expectancy for people with Marfan syndrome is now about the same as for people who don't have it. You might be aware that lots of people believe that Abraham Lincoln had Marfan syndrome and this could have been a contributor to his unusual height. Some people theorise that Tutankhamun and Julius Caesar may also have had this condition. For a short time about 10 years ago, there was a rumour going around that Michael Phelps, the Olympic swimmer, had Marfan syndrome, and this would have been particularly newsworthy because of the stress that his physical activity puts on his cardiovascular system. Well, it turns out not to be true, but this new story shone a big light on Marfan syndrome and its complications in children, especially children who are athletes and adults. There was also a 1984 Olympic silver medalist women's volleyball player named Flo Hyman, who had Marfan syndrome, and she died during a game from an aortic rupture in 1986.
0:12:29.4 RW: Because Marfan syndrome is a genetic disorder, there's no specific cure for it. People with cardiovascular issues are typically prescribed beta blockers and watched carefully for any signs of damage to heart valves or the structural integrity of the aorta. The eye problems associated with Marfan syndrome are usually treatable, but they have to be tracked, and the skeletal issues associated with Marfan syndrome, again, these can be treated if they're severe enough to cause pain and other problem. Specifically, that caved in pectus excavatum may need to be surgically corrected, because if it's very severe, it can put mechanical restrictions on how the thorax moves, and that can damage the lungs and lead to other really serious problems.
0:13:17.1 RW: So I learned from our contributor that she only saw this client one time and he has not returned, at least not yet. So she has not had a chance to develop an ongoing relationship with him. But if she does, I hope she'll get some information about the strength and resilience of his cardiovascular system, since problems with the heart and aorta are so common among patients with this condition. The fact that this client is using physical therapy for his history of injuries suggests that his capacity for exercise is pretty good and that's a great place to start. But in this kind of situation, more information is better than less. Let's also be aware that beta blockers have some side effects, including fatigue and cold extremities, and these might inform some of our decisions about massage therapy.
0:14:05.6 RW: If you have clients with Marfan syndrome, and you have found that they have special needs or requests related to the way it affects them, I'd love to hear about it. I would be delighted to do a follow-up I Have A Client Who episode on Marfan syndrome. Just let me know.
0:14:21.1 RW: Hey everybody, thanks for listening to I Have a Client Who, pathology conversations with Ruth Werner. Remember, you can send me your I Have a Client Who stories to ihaveaclientwho@abmp.com, that's ihaveaclientwho, all one word, all lowercase @abmp.com. I can't wait to see what you send me, and I'll see you next time.