
Student’s elbow? Popeye’s elbow? Whatever you call it, an infected olecranon bursa is no joke. Lots of people have to go through several attempts to treat it, culminating in surgery to remove it. When is massage therapy safe?
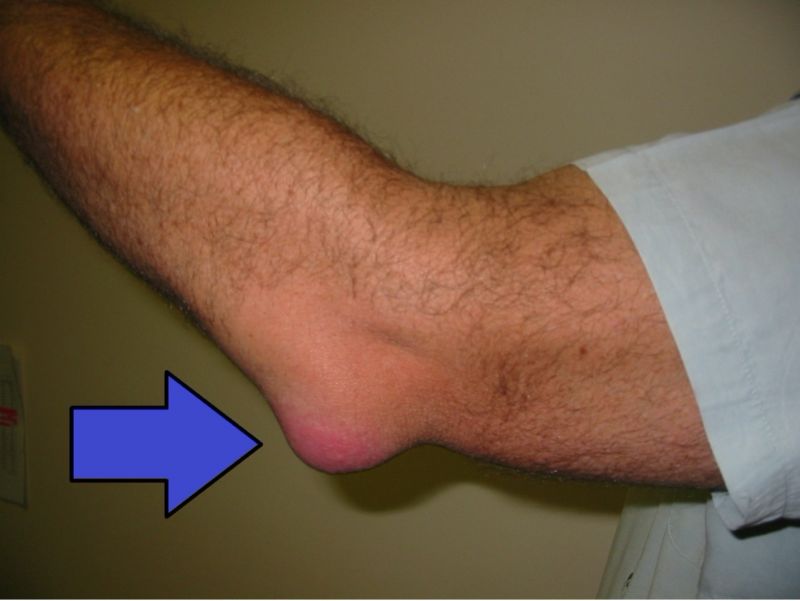
Infected olecranon bursitis
https://commons.wikimedia.org/wiki/File:Bursitis_Elbow_WCArrow.jpg


This podcast sponsored by:
About Anatomy Trains:
Anatomy Trains is a global leader in online anatomy education and also provides in-classroom certification programs forstructuralintegration in the US, Canada, Australia, Europe, Japan, and China, as well as fresh-tissue cadaverdissectionlabs and weekend courses. The work of Anatomy Trains originated with founder Tom Myers, who mapped the human body into 13 myofascial meridians in his original book, currently in itsfourthedition and translated into 12 languages. The principles of Anatomy Trains are used by osteopaths,physicaltherapists,bodyworkers,massagetherapists,personaltrainers,yoga,Pilates,Gyrotonics,and other body-minded manual therapists and movement professionals. Anatomy Trains inspires these practitioners to work with holistic anatomy in treating system-wide patterns to provide improved client outcomes in terms of structure and function.
Website:anatomytrains.com
Email:info@anatomytrains.com
Facebook:facebook.com/AnatomyTrains
Instagram: instagram.com/anatomytrainsofficial
0:00:00.0 Speaker 1: Ruth Werner's best-selling book, "A Massage Therapist's Guide to Pathology," is a highly regarded comprehensive resource that sets the standard for pathology education. Written for massage therapy students and practitioners, this ground-breaking resource serves up a comprehensive review of the pathophysiology, signs, symptoms, and treatment of more than 500 diseases and disorders. Learn more at booksofdiscovery.com.
0:00:32.2 Speaker 2: "Anatomy Trains" is happy to announce our return to the dissection lab in-person, January 10th to the 14th, 2022, at the Laboratory of Anatomical Enlightenment in Boulder, Colorado. We are thrilled to be back in the lab with "Anatomy Trains" author Tom Myers and master dissector Todd Garcia. Join students from around the world and from all types of manual, movement, and fitness professions to explore the real human form, not the images you get from books. This is an exclusive invitation. Email: Info@anatomytrains.com if you'd like to join us in the lab.
[music]
0:01:16.8 Ruth Werner: Hi, and welcome to "I Have A Client Who," pathology conversations with Ruth Werner, the podcast where I will discuss your real life stories about clients with conditions that are perplexing or confusing. I'm Ruth Werner, author of "A Massage Therapist's Guide to Pathology," and I have spent decades studying, writing about, and teaching about where massage therapy intersects with diseases and conditions that might limit our client's health. We almost always have something good to offer even with our most challenged clients, but we need to figure out a way to do that safely, effectively, and within our scope of practice. And sometimes, as we have all learned, that is harder than it looks.
0:02:02.0 RW: Today's "I Have A Client Who" story comes from a massage therapist in Ohio, who found me through Facebook Messenger while I was on vacation. I was unable to respond to her in real time, but I heard back from her later, as you will see. If you would like to send me an "I have a client who" story, you can do that on Facebook Messenger, or through my website, or through a dedicated email address, ihaveaclientwho@abmp.com. That's ihaveaclientwho, all one word, all lowercase, @abmp.com. It's amazing how often I have to shake the trees to look for these stories. I would love it if you would send me your stories and questions so that your experiences can enrich all of the people who listen to this fabulous podcast.
0:02:57.1 RW: In any case, today's story goes like this. "I have a concern. I have a client who wants an appointment. The client had a staph infection in the elbow bursa and surgery, and I haven't heard of that before. The client said the doctor said she is completely recovered. I can't get them in for two weeks. Is there any concern for giving a massage? What does the surgery consist of? Thanks for any information."
0:03:24.6 RW: What I told her, just briefly, was that she should find out if the client was still using antibiotics and if her doctor said it was safe for her to exercise. My thinking is that if the course of antibiotics has been concluded and the client is encouraged to exercise, then massage therapy, at least away from the surgical site, would be safe. Later, when I got home, I reached out to this therapist to find out whether she'd be willing to let me use her story for this podcast, and here's what she said. "I'd love it. She's off all antibiotics, and her doctor said she's under no restrictions. Thanks." So, all seems well for this client and this therapist to proceed safely, but the issue of infected bursitis at the olecranon is an interesting one, and I thought it deserved a little more attention.
0:04:16.1 RW: You will recall that we have bursae distributed all over our body, and they occur mostly at friction points and where attendants have to cross over sharp, bony corners. The purpose of bursae is to reduce friction, and to add some cushioning, and to generally be just a little bit of softening on our sharp edges. The bursae that occur at the tip of the olecranon have to provide a little bit of cushioning for when we lean our elbows on our desk or other surfaces when we work, but they also have to ease the work of the tendon of the triceps on its way to the proximal end of the ulna. We have bursae in lots of locations all over the body. The one that turns up most often in the context of massage therapy is the subacromial bursa, and that inhabits the space between the acromion and the head of the humerus. When that bursa is inflamed, any movement, passive or active, tends to be painful, so painful that it becomes difficult to move the arm freely, especially in abduction.
0:05:18.0 RW: We have several bursae all around our knee, both to cushion that bony corner and to allow for better freedom of movement of the patellar tendon and ligament structures. When some combination of these bursae become inflamed, this is sometimes called a "housemaid's knee," because it's associated with people who are on their knees a lot. There's a big bursa on the lateral aspect of the trochanter, and trochanteric bursitis is responsible for a fair amount of misery. There's even a bursa internally, where the iliopsoas needs to be cushioned anterior to the hip joint capsule, and bursitis there can have a big impact on a person's ability to walk. We can grow new bursa if we need to, which turns out to be really useful because sometimes it is necessary to surgically remove these structures. And we see within several months that they tend to grow back, and isn't that amazing?
0:06:15.9 RW: Bursitis at the olecranon has a couple of different names. I have always learned it as "student's elbow," because you can imagine the posture of a student at a desk, propping their chin up on their elbows, very studiously reading from a book. But I learned as I was preparing for this podcast that it has another name, which is called "Popeye's elbow," and that refers to the big bulge at the very tip of the olecranon that looks like a cartoon of Popeye. I found a nice picture of the kind of olecranon bursitis we're talking about today on Wikimedia, so I will include that photograph and a link in our show notes.
0:06:57.6 RW: But it turns out that the bursa at the olecranon is also especially vulnerable to becoming inflamed not because of overuse or irritation, like we saw with that massage therapist, but because of the risk of infection. Any trauma that compromises the skin at the tip of the elbow, and this could be a scrape or an insect bite or being scratched by a thorn as you work in the garden, really anything that breaks the skin at the tip of the elbow introduces pathogens into that area, and we run the risk of having those cooties take up residence inside the bursal sac, where they are essentially protected. And the net result is that the bursal sac swells up like crazy, and the tip of the elbow becomes inflamed and red and fabulously painful.
0:07:49.6 RW: The basic treatment for this kind of infection is to start with oral antibiotics. But it's actually not unusual for this to be unsuccessful, because these pathogens are hiding in a place without a big blood supply, and it's hard for the drugs to get access to them. This bursa might then be aspirated in the hopes of pulling out enough infected fluid that the bursa can heal. Sometimes cortisone is injected into the bursa in an attempt to de-inflame it and help it to heal. But for a lot of people, these interventions also don't work. The bursa re-inflames, continues to be infected, and they continue to have pain and limitation. So, for a certain number of patients who have a bacterial infection at the bursa, at the point of the elbow, they need to have the whole business surgically removed, which was the situation for the client in today's story.
0:08:44.7 RW: If this client had somehow convinced her massage therapist to work with her before being fully treated for her infected olecranon bursa, it is not terribly likely but is definitely within the realm of possibility that massage might have disrupted this infection to the extent that she could have had staph bacteria move to other places in her body. Because let's remember that while there may be a colony of bacteria growing inside the bursal sac, there could also, in fact it's likely, that there are bacteria inhabiting the cells and interstitial spaces all around the area as well. Massage therapy anywhere close to this neighbourhood could be disruptive and, of course, that's not a great outcome. The massage therapist was definitely correct in wanting to delay any massage until treatment for this infection was complete.
0:09:37.4 RW: So now a couple of weeks later, the client has finished with her surgery, and she's finished with her antibiotics, and she's been cleared for all activities. And this is a great time to include massage therapy as part of her recovery, especially if this massage therapist has any education in working with scar issue. Because at this moment, gently mobilising and working with the area around the elbow surgery could contribute to an even more successful treatment outcome.
0:10:08.2 RW: It was a pretty simple story today with some interesting things to consider, but really nothing here that strained our critical thinking machine. Still, infected olecranon bursitis turns out to be fairly common, and my guess is that it may be even more common in summertime, since we're working and playing outside, and elbows are more likely to be injured. So, I wanna offer my thanks to this massage therapist who gave me an easy job this week, and I wanna offer my thanks to you for tuning in for one more episode of "I Have A Client Who."
0:10:41.2 RW: Hey, everybody, thanks for listening to "I Have A Client Who" pathology conversations with Ruth Werner. Remember, you can send me your "I have a client who" stories to ihaveaclientwho@abmp.com. That's ihaveaclientwho, all one word, all lowercase, @abmp.com. I can't wait to see what you send me, and I'll see you next time.