

Going for Gold
A gold medal-winning massage may not be what you think. It’s not about fancy tools, flashy techniques, or pedigree. It’s about centering the bodywork on the client experience.
There is much we don't know about temporomandibular joint dysfunction (TMD or TMJD). Although sometimes clearly the result of an injury, in most cases, we don't know what causes TMD and its associated pain, tenderness, and movement issues. Although an estimated 40-75 percent of adults show at least one TMD sign at some point in their lives (for example, about 50 percent of adults have nonpainful jaw noise or asymmetrical movement), we don't know why only about 33 percent of those adults ever experience pain or dysfunction. We don't know why people over age 60 very rarely complain of TMD, or why the most severe sufferers are up to nine times more likely to be female than male, or why many TMD patients experience other systemic conditions that also affect more women than men, such as chronic fatigue syndrome, fibromyalgia, generalized pain conditions, rheumatoid arthritis, interstitial cystitis, vulvodynia, endometriosis, or irritable bowel syndrome.1
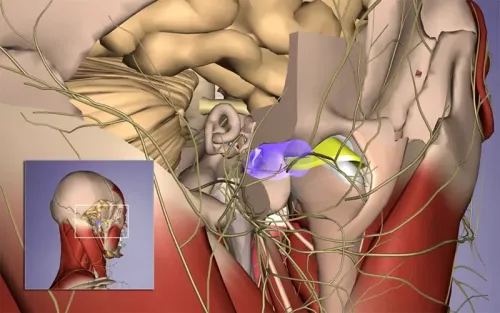
We do know that TMD often seems to have mechanical aspects, referred to as axis I in the most common diagnostic system—the Research Diagnostic Criteria for Temporomandibular Disorders.2 These physical aspects include tissue inflammation, disc displacement, excessive laxity or tightness of the joint, and the most common axis I feature—myofascial pain.3 Just as importantly, we know that TMD is frequently correlated with psychological factors (axis II) such as anxiety, depression, mental or emotional stress, or sympathetic (fight-or-flight) autonomic nervous system (ANS) arousal.4 As a result, there is wide agreement that TMD assessment and management should include both physical and psychological support.5
Although chronic TMD sufferers may respond best to an integrated approach combining multiple disciplines (since TMD can involve many factors), several large-scale studies show that manual therapy can often help TMD, alone or in combination with other methods.6 In our Advanced Myofascial Techniques approach at Advanced-Trainings.com, we have found that hands-on work can frequently help TMD in several ways—both by skillfully addressing the above-listed axis I mechanical contributors, and through the nonmechanical effects of hands-on work. These effects include increased proprioceptive refinement, shifts in pain perception, and promoting relaxation and nonpainful body awareness through calming effects on sympathetic ANS arousal (such as stress responses, mental agitation, posttraumatic stress disorder, etc.).
I described several techniques for working with the anatomical and mechanical contributors of TMD in the three-part series "Working with TMJ" (Massage & Bodywork, July/August, September/October, and November/December 2009, later expanded and updated in Advanced Myofascial Techniques, Volume 2, Handspring, 2016). In the box at left, I offer two additional gentle techniques that focus on the proprioceptive or neurological aspects of jaw tension and coordination.
Try them out, but rather than using them as physical manipulations, joint mobilizations, or fascial stretches, imagine these two techniques as gentle but effective ways to calm your client's nervous system arousal level, relax excessive unnecessary muscle tension, and increase body awareness.

"Fly Landing" variation (Image 3): use the lightest possible touch on chin (no more than 2 grams of pressure) in order to draw client's awareness to any tension that would resist jaw depression (opening). Do not push on jaw, but instead, invite client to relax and breathe.

"Horseshoe Grip" variation (Image 4): with very soft hands, cradle the occiput and mandible with a "horseshoe" (curved) grip. Encourage client relaxation, as you slowly and gently motion-test for subtle side-to-side and depression/elevation jaw ease. Stay well within the client's comfort range, inviting relaxation and ease (support and wait, instead of mobilize—do not stretch, move, or use pressure when the client has acute pain or guarding).

1. R. K. Ow et al., "Symptoms of Craniomandibular Disorder Among Elderly People," Journal of Oral Rehabilitation 22, no. 6 (June 1995): 413-19; The TMJ Association, "TMJ Science Overview" (January 7, 2016), accessed November 2016, www.tmj.org/Page/51/32.
2. R. Wassell et al., Applied Occlusion (London: Quintessence, 2008): 73-84.
3. Look, John O. et al, "Reliability and Validity of Axis I of the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) with Proposed Revisions," Journal of Oral Rehabilitations 37, no. 10 (2010): 744-59. https://doi.org/10.1111/j.1365-2842.2010.02121.x.
4. Look, John O. et al, "Reliability and Validity of Axis I of the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) with Proposed Revisions." https://doi.org/10.1111/j.1365-2842.2010.02121.x.
5. D. Manfredini et al., "Research Diagnostic Criteria for Temporomandibular Disorders: A Systematic Review of Axis I Epidemiologic Findings," Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 112, no. 4 (2011): 453-62. https://doi.org/10.1016/j.tripleo.2011.04.021.
6. L. J. Pereira et al., "Psychological Factors and the Incidence of Temporomandibular Disorders in Early Adolescence," Brazilian Oral Research 23, no. 2 (June 2009): 155-60, http://dx.doi.org/10.1590/S1806-83242009000200011; M. S. Medlicott and S. R. Harris, "A Systematic Review of the Effectiveness of Exercise, Manual Therapy, Electrotherapy, Relaxation Training, and Biofeedback in the Management of Temporomandibular Disorder," Physical Therapy 86, no. 7 (July 2006): 955-73, https://pubmed.ncbi.nlm.nih.gov/16813476/; L. B. Calixtre et al., "Manual Therapy for the Management of Pain and Limited Range of Motion in Subjects with Signs and Symptoms of Temporomandibular Disorder: A Systematic Review of Randomised Controlled Trials," Journal of Oral Rehabilitation 42, no. 11 (November 2015): 847-61, https://doi.org/10.1111/joor.12321; S. Armijo-Olivo et al., "Effectiveness of Manual Therapy and Therapeutic Exercise for Temporomandibular Disorders: Systematic Review and Meta-Analysis," Physical Therapy 96, no. 1 (January 2016): 9-25, https://doi.org/10.2522/ptj.20140548; The TMJ Association, "TMJ Science Overview."
7. The TMJ Association, "TMJ Science Overview" (January 7, 2016), accessed November 2016, www.tmj.org/Page/51/32.
A gold medal-winning massage may not be what you think. It’s not about fancy tools, flashy techniques, or pedigree. It’s about centering the bodywork on the client experience.
Energy work can be a divisive topic in the massage field, however, there are valuable potential benefits and insights to be gained through exploring and integrating energetic modalities in therapeutic practice.
Time perception is shaped by interoception and body state, which means hands-on work can directly influence how clients experience duration.
By recognizing the knee as a transmission point within the kinetic chain rather than a standalone joint, therapists can address the upstream and downstream restrictions that can cause knee stress and pain.